Mixed Rebreather & Open Circuit Teams
Published in X-Ray MagazineIssue 105, June 2021
Text and Photos by Michael Rothschild
Click here to download published article PDF

INTRODUCTION
With the increasing popularity of rebreathers, it is becoming more and more likely that an open circuit (OC) diver will be buddied up with someone on a closed circuit rebreather (CCR). This may be a regular team, or a buddy pair formed when two people who are vacationing alone decide to dive together. It is even possible that an OC diver will encounter a rebreather diver from another team, and rescue or assistance might be necessary. This review came out of an online discussion of helpful things for a relatively inexperienced OC diver to know about CCRs. It is NOT intended to be a comprehensive introduction to rebreathers, but rather a quick overview of things that an OC diver should learn to be a safe member of a mixed OC/CCR team. Also, I'm assuming here that any safe team will discuss gas and dive planning ahead of time based on the individual limits of each member, that's not what this article is about.
Some rebreathers are of the semi-closed design (SCRs), which work differently than CCRs. For the sake of clarity, I have used the abbreviation CCR throughout this article, but much of this applies to SCRs as well.
Please remember that rebreathers are much less standardized than open circuit gear, and there is a wide range of equipment configurations and procedures in use. For the purpose of simplicity, I am considering a common CCR setup for recreational diving within no-decompression limits (NDL). It is true that some CCR divers have complex gear such as special gasses that are unsafe to breathe in shallow water or multiple bailout tanks. However, it is fairly unlikely that such a diver would be in a mixed team with the OC diver for whom this article is intended.
It would be confusing and counterproductive to try to cover all possibilities in an article of this scope. Therefore, any mixed dive team MUST have a thorough discussion before entering the water about the specific gear configuration being used, and the expectations for each team member during the dive and in an emergency.
One thing to know about CCR divers is that we love to talk about our gear at all times EXCEPT during our pre-dive checks. If you see a diver breathing through their rebreather on a dive boat, don't ask them questions, and if you do, don't assume they are rude if they don't answer. This is the “pre-breathe” – several minutes of breathing through the unit before entering the water, to make sure that all systems are working well. Even before or after the pre-breathe, there are a number of things on the checklist that we may be going over, and that's not the time to be chatty.
REBREATHER BASICS FOR OC DIVERS
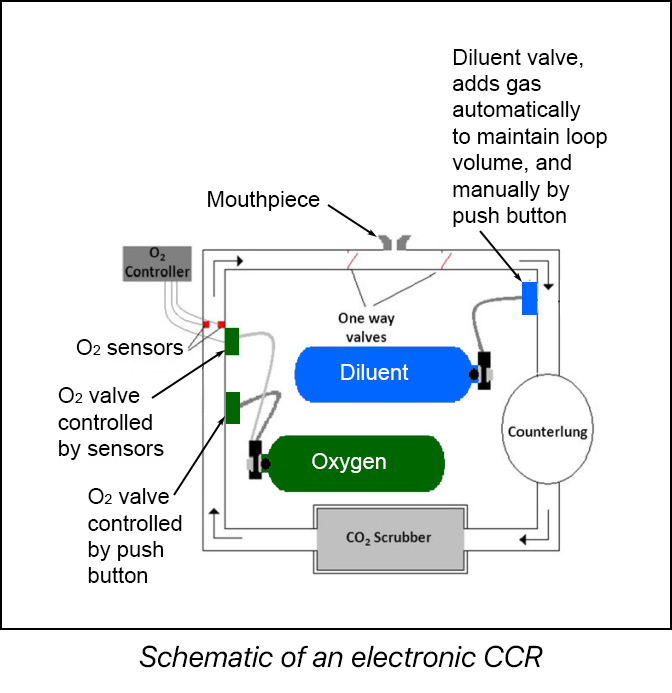
From the point of view of an OC buddy in a mixed team, there are a few basic CCR concepts that are important to know. A CCR works by circulating a single breath in a closed pathway (the “loop”) in which there is a container of a chemical (a “scrubber”) that removes the carbon dioxide (CO2) that the diver produces. The machine also has the ability to add gas from two tanks into the loop: pure oxygen (O2) and “diluent” (which may be air). The O2 replaces oxygen consumed by the diver, while the diluent keeps the loop filled with gas as depth and ambient pressure increases. By the appropriate addition of these two gasses, the rebreather diver is able to maintain the partial pressure of oxygen (PO2) in the loop in the breathable range – too high or too low is lethal.
Once again, this is not meant to be a comprehensive overview of rebreathers – there are different types of rebreather design, and I have simplified the diagram by showing something called an eCCR (electronic CCR) in which oxygen addition is partially controlled by a computer that monitors oxygen sensors. Other designs involve the continual flow of oxygen into the loop and reliance on the diver to manually replace consumed oxygen (mCCR).
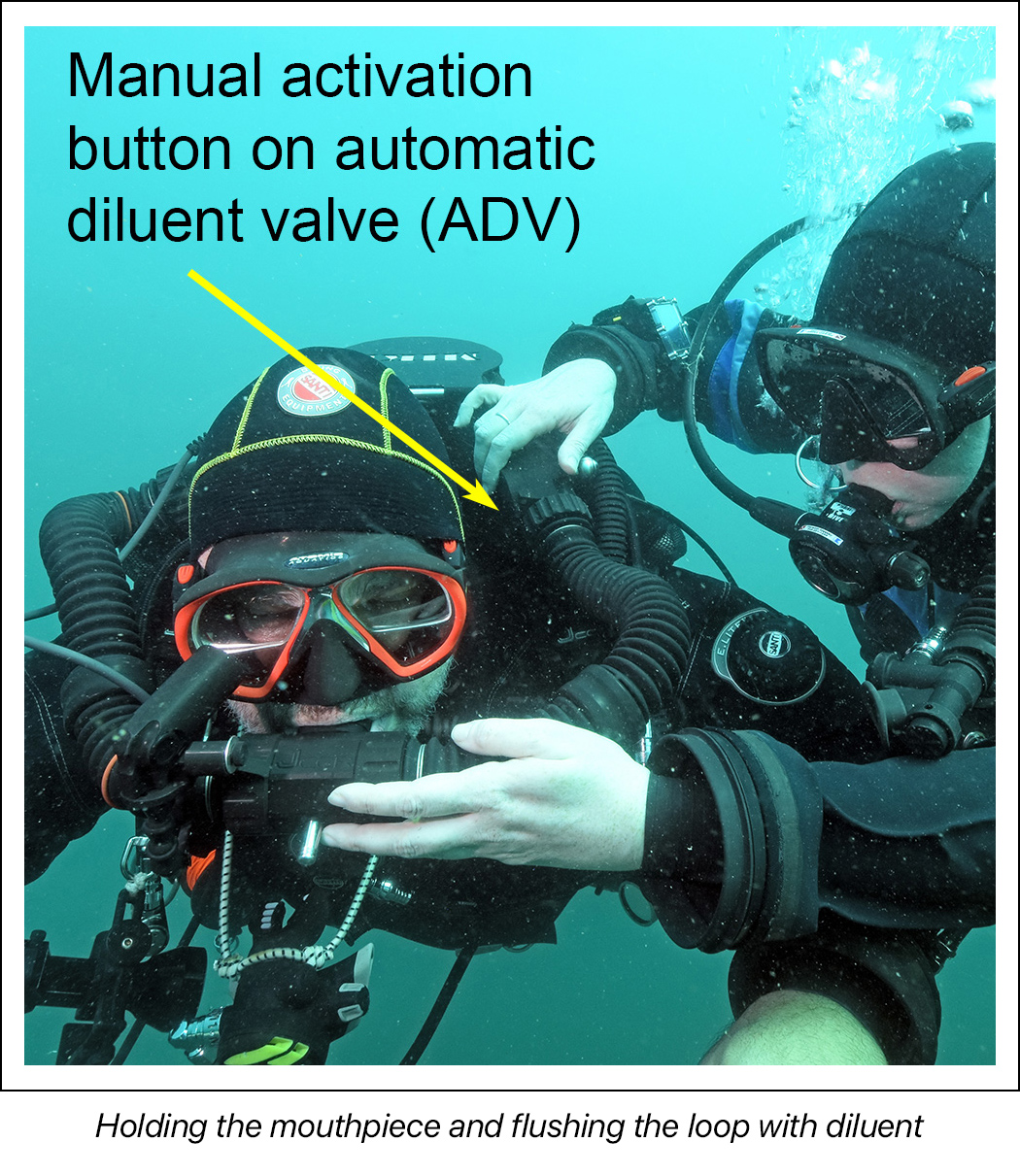
But with any design, there will be a button somewhere to allow the manual addition of diluent to the loop. This may be on the ADV (automatic diluent valve, which adds gas as needed to compensate for increased ambient pressure), or on a separate manual addition valve (MAV). This is probably the most important control for the OC diver to understand. Some CCRs have an inline shutoff valve on the ADV gas supply hose; this must be opened if you are going to use the ADV button to add diluent to the loop. There will also be a MAV for O2, in addition to some method of automatically adding oxygen.
During the pre-dive discussion, the CCR diver will show you where these buttons are. It is crucial to remember which is which. As we will see below, in some emergencies you might add diluent for an unresponsive diver, but NEVER oxygen, which can cause life threatening spikes in oxygen levels. Adding diluent will ALWAYS introduce fresh gas of a known, safe composition into the loop. The only exception to this rule would be “hypoxic diluent”, which doesn’t have enough oxygen to support life in shallow water, but as mentioned above, that is beyond the scope of this article.
Flushing the loop with diluent can help in situations where the oxygen levels are too low or high, or where there is a buildup of excessive CO2 in the loop. Remember that this will also add buoyancy to the CCR diver and therefore will require venting of the loop. Discuss this option with your buddy ahead of time.
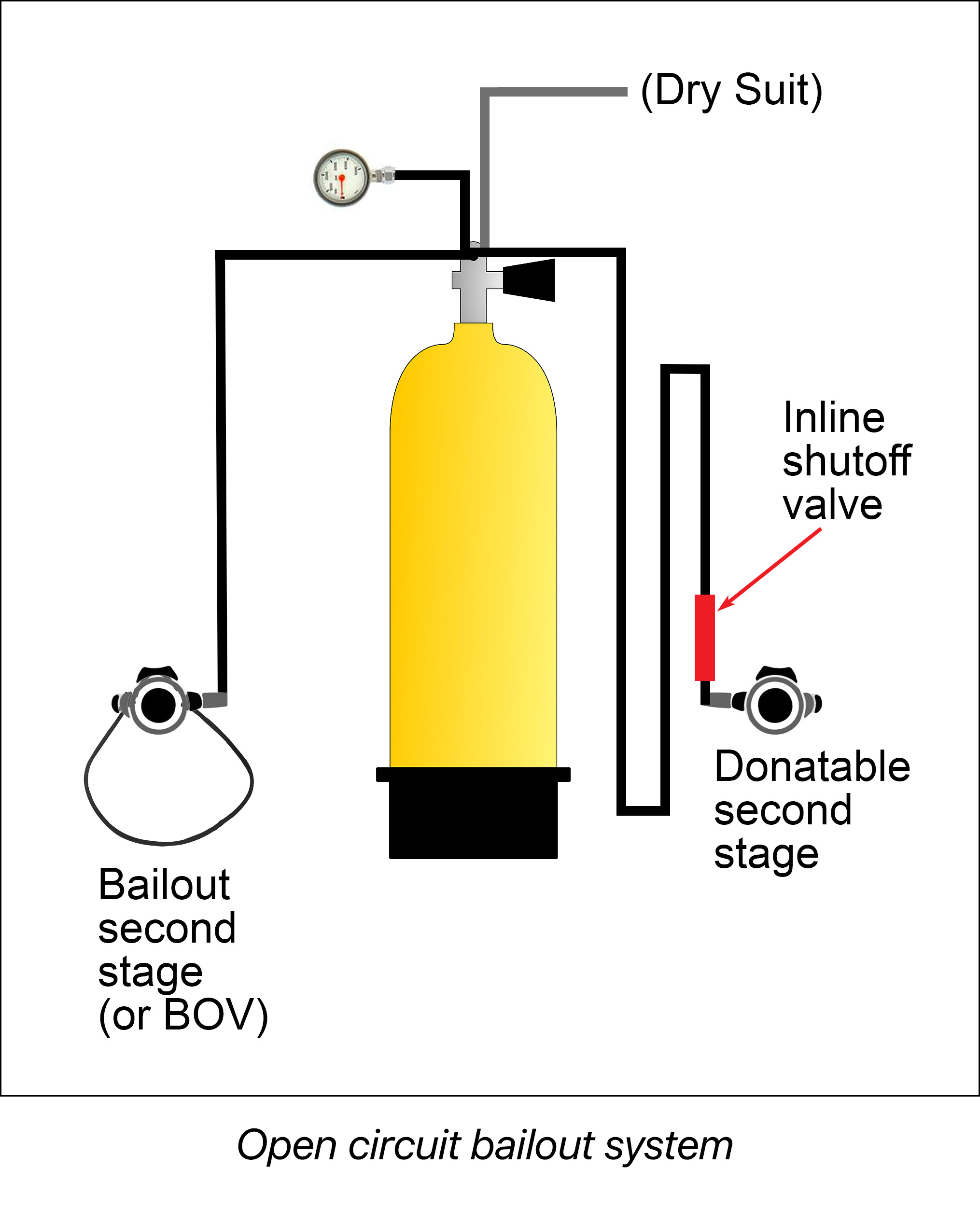
The term “bailout” refers to a complete, independent OC system carried by rebreather divers – a tank with a first and second stage regulator. In some designs, bailout and diluent come from the same gas source, and there may be multiple tanks for different depths, but the idea is that the system will always supply breathable gas no matter what is happening with the rebreather itself. The bailout system has to have enough gas to allow for a safe ascent if the rebreather became unusable for any reason during the dive.
In rebreather training, there is a low threshold for getting off the loop and onto this backup OC system – “When in doubt, bail out!” This is especially important since some of the problems that CCR divers can have related to gas problems in the loop are first detected by a strange feeling that something is not right. Bailing out early can be life-saving in this situation. Often, this lets the rebreather diver fix something that will let them return to the loop and finish the dive, but enough gas must be carried to reach the surface on OC alone if necessary.
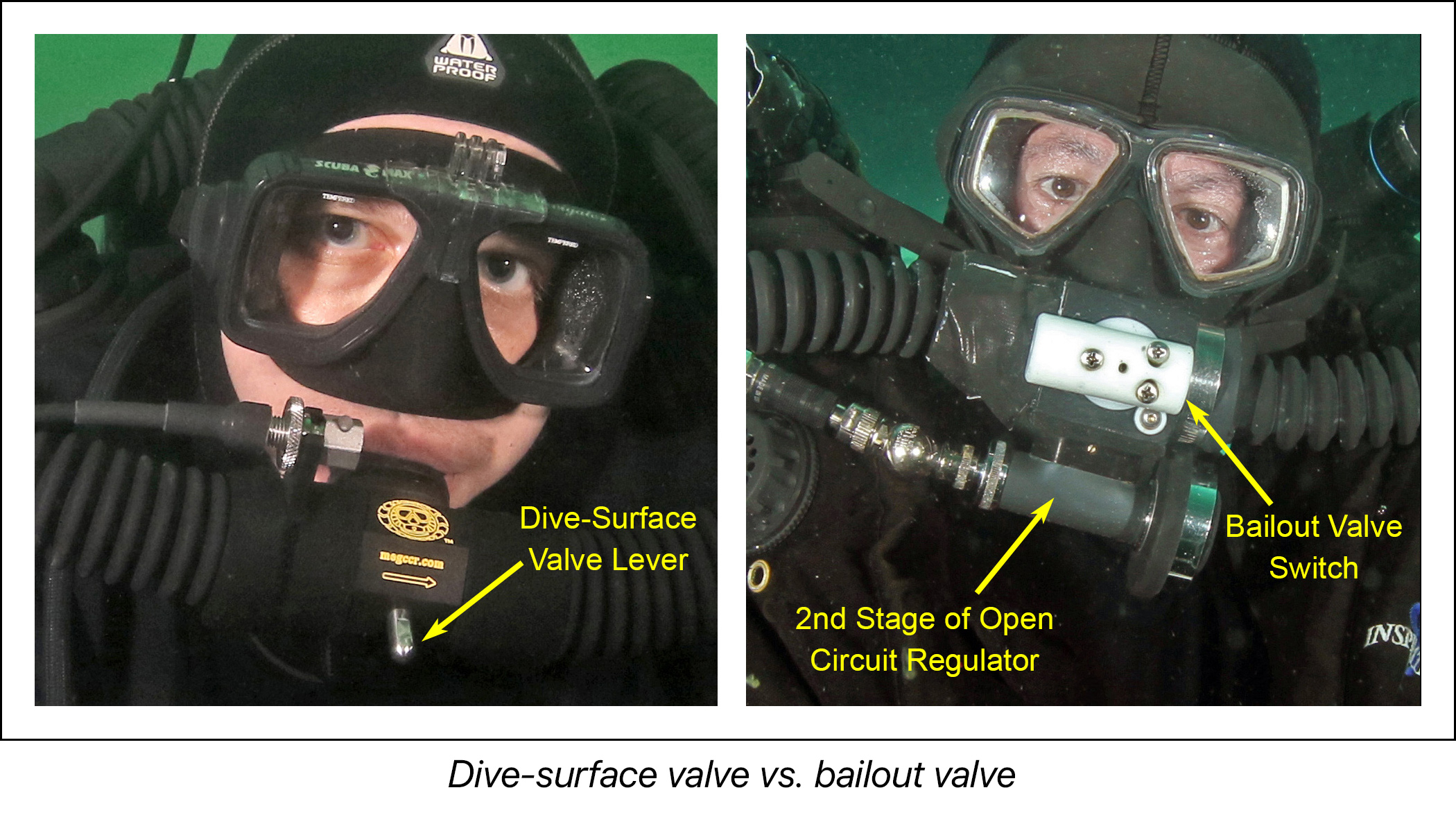
Switching from breathing through the loop to breathing from the bailout tank may be done in two ways, corresponding to two different designs for the CCR mouthpiece. The simplest design is the dive-surface valve (DSV). This is a switch that closes off the loop from the mouthpiece – it must be open to breathe from the loop, but closed whenever the loop is out of the diver’s mouth to keep from flooding the rebreather. Divers using a DSV have a standard OC regulator connected to the bailout (often bungeed under the diver’s neck or to the tank). When bailing out, they close the DSV and switch to this regulator.
Another option is something called a bailout valve (BOV). The BOV consists of an OC regulator built into the loop, but connected to an alternate source of gas. The regulator and the loop share the same mouthpiece, and the switch connects the mouthpiece to either the loop or the regulator. With a BOV, you bail out by throwing the switch without removing the loop from your mouth, which connects the mouthpiece to the OC regulator AND seals off the loop. This is faster than bailing out from a DSV, with less of a chance of flooding the rebreather.
BEFORE THE DIVE
The first thing to determine is if a mixed OC/CCR team is appropriate in the first place. Neither diver should feel pushed into doing this if they don’t feel comfortable with the concepts outlined in this article. Yes, there are a lot of complex details to be learned that are far beyond what is required for recreational certification, but any OC diver attempting this is absolutely obligated to put in the effort to understand these basic concepts. Similarly, it is NOT a good idea for a very new OC diver to be the sole buddy for a rebreather diver. Anyone diving in a mixed team needs to be very comfortable with their own diving skills and equipment.
While all buddy teams should go over plans and protocols before splashing, this discussion is especially important for a mixed OC/CCR team. Time should be allowed so that the OC diver is not rushed, and can fully understand the implications of diving with a rebreather diver. Specific details of the CCR gear being used must be reviewed.
During the pre-dive discussion, It’s a good idea for the CCR diver to let the OC diver physically throw the BOV or DSV switch – these can be fairly stiff and require some effort to use. The OC diver should also try pushing the ADV or diluent MAV button, opening up the inline shutoff if present, and both inflating and deflating the CCR wing. Overpressure dump valves for both the wing and the counterlungs should be identified as well.
In a mixed team, there needs to be enough bailout gas to handle a wide range of emergencies, including gas sharing with the OC diver. While planning such a dive, a discussion should be had about the amount of bailout carried. While it is unlikely that both divers would need an alternate gas source, in an emergency, air consumption goes way up. Some recreational CCR divers only carry a 40 cubic foot aluminum tank, and some gear configurations involve a single tank that provides both diluent and bailout. An aluminum 80 is a common choice for bailout to provide an extra margin of safety, especially for a team that includes OC divers.
So what do we do if the OC diver needs gas? Again, this is something to discuss ahead of time. Many OC divers are trained in the standard “primary donate” technique, in which the rescuing diver gives the working regulator that they are breathing from to the victim. This is NOT done when the rescuer is on CCR. I don’t have a BOV, so I could give you my OC bailout regulator, which is bungeed around my neck. However, then I would have no bailout available, which is not ideal. It is also on a fairly short hose. In an emergency, with an immediate ascent and no deco obligation, this could work. But there are better options.
One approach to this problem is to put a second regulator on a long hose on the bailout tank. When I go through my pre-dive review with an OC buddy, I show them how I would donate gas. BOV divers usually also have an OC regulator bungeed to their bailout tank, in case of a problem that affects the BOV itself (like a mouthpiece that is torn, lost or contaminated with caustic chemicals from the scrubber).

Unlike the deco bottles carried by OC tech divers, which are usually carried charged but with the valves shut off, many CCR divers leave their bailout tank valves open. The idea is that in a CO2 emergency, your dive skills are significantly degraded, and panic with hyperventilation can make it very difficult to get off the loop. This is an advantage of the BOV, which gives you OC gas at the throw of a switch.
Because of this open valve, divers carrying an extra regulator will sometimes put an inline shutoff switch before the second stage, to prevent an unnoticed free flow with gas loss. The OC diver needs to ask if this switch is present, and to make sure that they know how to open it in an emergency.
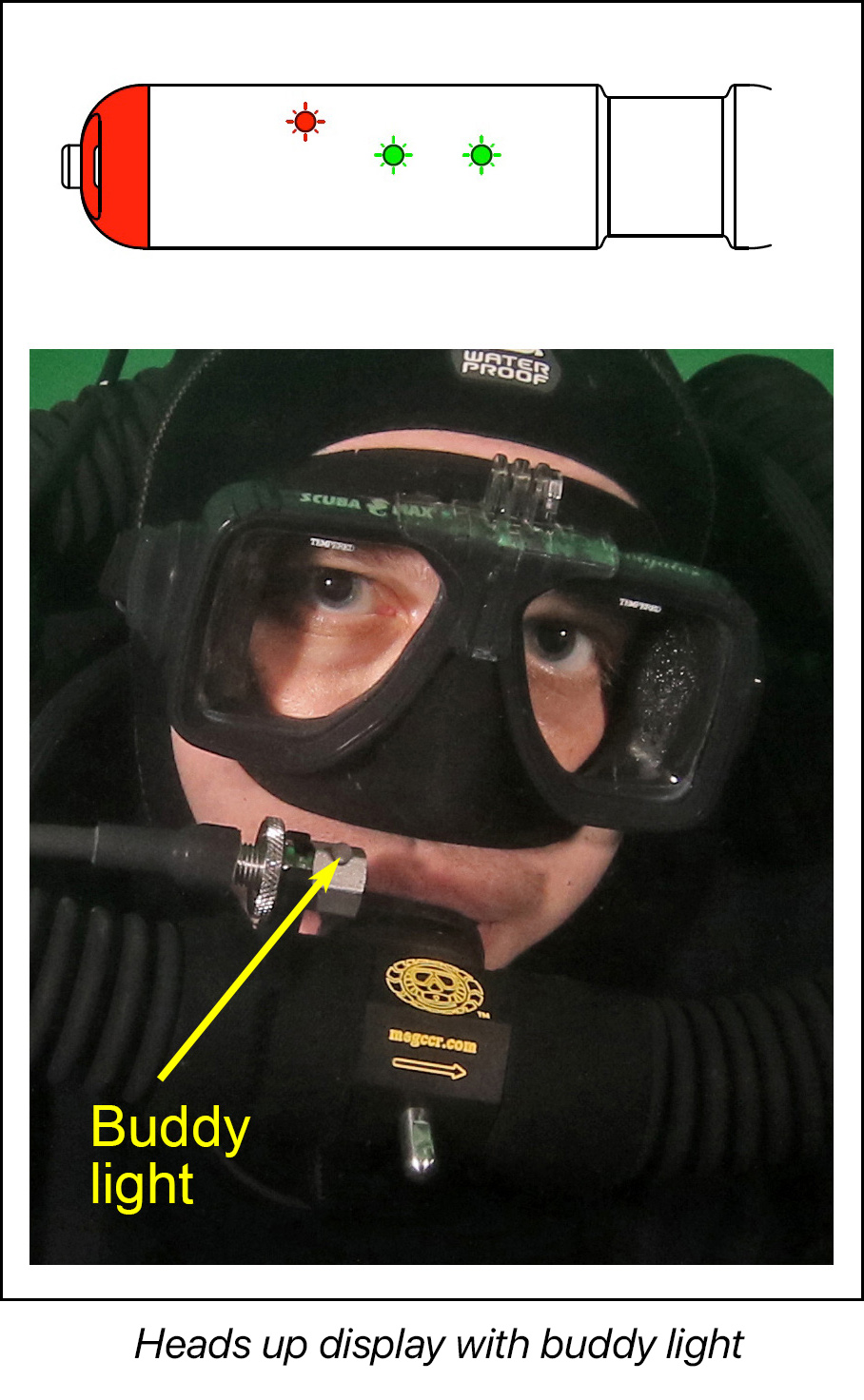
Ask about the significance of a flashing red light, or any other sound or visual alerts on your CCR buddy's handset or heads up display (HUD, attached to the loop). Usually, this means that the oxygen levels are too low or too high. There have been cases where a buddy noticed this before the diver did, and called attention to it!
The CCR diver should let the OC diver know about routine rebreather procedures that they may do during a dive, so that the OC diver doesn’t think that there is an emergency or a problem. Of course, communication during the dive can help with this - the CCR diver should give the “I’m OK” sign before doing anything unplanned. But it is helpful to inform the OC buddy about a potential diluent flush, O2 flush at 20 feet on descent or ascent, and any drills (e.g. loop recovery, bailout, etc..) that might be done.
DURING THE DIVE
If conditions permit, once both divers are in the water on the surface, a quick bubble check is a good idea. Have the CCR diver submerge the unit by leaning backwards, and look underwater for any obvious gas loss before starting the dive.
Rapid descents - which are fine on OC - can cause an O2 spike on CCR, so they are avoided. If the OC diver is leading and drops rapidly in poor visibility conditions, buddy separation becomes more likely. This problem is made worse for the OC diver, since there will be no bubbles to help find a missing buddy. Descents and ascents in general require more active management on a CCR than on OC, so the OC diver should pay special attention during these times of task loading.
CCR divers usually do a bubble check at around 20 feet, and may spend a minute or two testing their monitoring systems. Make a point of looking at your buddy’s rebreather from top to bottom, and on all sides, before continuing with the dive. There are a lot of places where gas can leak (especially fittings like the ADV, MAV, main canister and first stages), and it is important to look for any bubbles again, since some leaks may not be apparent on the surface. There should be no significant gas escape on descent.
This is also the time to look at the CCR diver’s overall gear appearance. Look for excessive mobility of the rebreather or bailout tank on the diver, and look for anything hanging loose. The CCR diver may also do an oxygen flush at this point (some do it a 20 feet on ascent), to make sure that their sensors can read a high PO2.
One thing to remember is that sawtooth profiles are generally avoided by rebreather divers. This is because descents require adding gas to the loop, and ascents require venting. This wastes gas from the small reserves on a rebreather, and also requires buoyancy adjustments and extra management of the PO2, which changes with depth. Rebreather divers tend to maintain a constant depth and swim around objects rather than over and under them when possible.
Rebreather divers also try to avoid heavy exertion, to avoid overtaxing the scrubber. While there are a number of factors that determine the scrubber’s efficiency, CO2 production is tied to the workload, and it is possible for dangerously high levels of CO2 to build up if the diver works too hard.
During an ascent, the CCR diver will have to vent the pressure of expanding gas in the loop, so you will see bubbles. They usually come from the diver’s mask, but also may come from around the mouthpiece or from an overpressure valve. This is normal.
IN THE EVENT OF EMERGENCY
An unconscious diver on OC will rarely survive, although many OC divers learn techniques to attempt rescue. The basic principles of this still apply to an unconscious CCR diver (getting the victim to the surface quickly, keeping the mouthpiece in the mouth, allowing gas to escape from the airway on ascent, etc.). However, survival may be actually more likely with CCR - one study [1] of French military rebreather divers who used a gag strap (to keep the loop in place) found that 51 of 54 divers who lost consciousness at depth surfaced successfully!
Remember that there is a difference between distracted, confused, unresponsive, and unconscious. A distracted diver will respond to standard communication. A confused diver may respond to aggressive stimuli (e.g., touching or light signals directed at the mask). In some types of CCR accidents, a diver may be conscious but unresponsive - such as with a low PO2, elevated CO2, or after a seizure. If they are using a full face mask, a gag strap or another mouthpiece retaining device, they may well be completely unconscious but still breathing fairly normally.
If the unresponsive diver has the loop out of their mouth, the first thing to do would be to attempt to insert an OC regulator (yours or theirs). The other thing that is vital to do immediately is to close the DSV or turn the BOV to OC mode. Although the rebreather may be partially or completely flooded at this point from water entering through the mouthpiece, closing the loop will prevent it from flooding more than it already has. A flooded rebreather will be very negatively buoyant and making rescue much more difficult. Of course, in this situation the chance of a successful rescue is small.
If the loop is in place, keep it in the diver’s mouth. If a BOV is present, throw the switch to the OC position, and bubbles should appear if the diver is breathing. If a BOV is not present, keep the loop in the diver’s mouth, but NEVER throw the DSV switch (remember, the DSV seals off the loop and the diver won’t be able to breathe). You can flush the loop with diluent in this situation, using the ADV or diluent MAV. If you do this, be prepared for increased buoyancy, and vent through the overpressure valve. The specifics of this are very important, and should be discussed ahead of time, but remember that you should NEVER throw the switch on a DSV while the loop is in the diver’s mouth, and you should NEVER flush with O2.
One catastrophic consequence of excessive oxygen exposure is a seizure. It is not the seizure itself that is dangerous, but the loss of the loop with unconsciousness. A standard recommendation is to hold the loop in the victim’s mouth and wait until the “clonic phase” of the seizure (shaking) has stopped before ascent. This is for two reasons. First, it would be much harder to manipulate a diver during a seizure. Second, during a seizure the airway may be closed, putting the diver at risk for severe pulmonary barotrauma on ascent.
Lifting an unconscious rebreather diver is particularly challenging, because of the increased possibility of runaway ascent due to expanding gas in multiple closed spaces. Also, it may be hard to for the rescuer to position themselves behind a bulky rebreather so as to hold the loop and manipulate the inflator hose at the same time. Being slightly above the victim (behind the diver’s head instead of directly behind their back) may be helpful.
In addition to venting gas from your own wing and the victim’s wing (as well as both dry suits, if used), you will also need to vent gas from the victim’s CCR loop. If a BOV is being used, remember that even though they may be breathing, the loop is now sealed off and won’t vent through the mouthpiece. The overpressure valves can help, but be aware of this issue. The way to avoid a runaway ascent is to be proactive with venting by pulling the dump cord (if present) or BRIEFLY opening and then closing the DSV if it is out of the diver’s mouth, with the mouthpiece held above your head. To make buoyancy matters worse, as you ascend, many CCRs will try to maintain the dropping PO2 by injecting oxygen into the loop. A rebreather diver ascending on OC will set the rebreather to “low setpoint” and/or shut off the O2 valve to make this less of a problem. If you are rescuing a CCR diver who is on an OC regulator (loop out or BOV), the O2 valve should be closed for this reason.
Don’t wait to dump gas until the runaway ascent has already started, with you trying to manage five different gas filled spaces simultaneously! Completely empty your wing and use the victim’s wing for buoyancy on ascent if needed (especially if the CCR has flooded). That way, if you lose your grip, the victim will at least surface.
Once on the surface, achieve positive buoyancy by inflating the wing, remove the loop and keep the victim’s mouth above the surface. You MUST remember at this point to close the DSV or switch the BOV to OC if it is not already in that position. If this is left open after removal from the victim’s mouth, the CCR can flood and become negatively buoyant, and the victim may sink even with gas in the wing. After reaching the surface, rescue is similar to that taught elsewhere. If the boat is immediately available, get the diver out of the water right away and activate the medical evacuation system. If a surface swim or pickup is needed, the rescuer should remove their own gear first and give rescue breaths while transporting the victim.
SUMMARY AND CHECKLIST
I hope that this article will help all members of a mixed OC / CCR team think about the discussions that should happen before getting in the water. I also hope that this basic introduction to rebreathers, while brief and superficial, will be enough to let a reasonably experienced and committed OC diver understand why these special techniques and protocols are necessary. I don't mean to scare people away from doing this, but each diver must realize that they are obligated to go beyond the standard diver buddy arrangements that they may have had in the past.
Here are a few basic questions that an OC diver should go over with a CCR buddy before the dive, in the form of a checklist. Remember, good communication is crucial for all dive buddies, but particularly in mixed OC/CCR teams.
1) What is your bailout configuration, dive-surface valve (DSV) or bailout valve (BOV)?
2) What would you like me to do if I find you truly unresponsive but with the loop in your mouth? If the answer is switch the BOV, then can I try doing that now?
3) Are there any depth considerations for your bailout gas(es) or diluent that I should know about?
4) Do you have an open circuit regulator that you could donate to me in case I have a catastrophic gas loss?
5) Where is your ADV or diluent manual addition valve (MAV)? Under what circumstances would you want me to push either of those buttons? Can I try doing that now?
6) Where is your wing inflator and dump valve?
7) Where would I look for high or low PO2 alerts on your heads-up display (HUD) or controller?
8) Is there anything that I should never touch or do?
REFERENCES:
1) Gempp, Louge, Blatteau, Hugon. Descriptive Epidemiology of 153 Diving Injuries With Rebreathers Among French Military Divers From 1979 to 2009. Military Medicine, 176, 4:446, 2011